East Melbourne VIC 3002


Vaginal thrush is a common infection caused by a yeast. 90% are candida albicans. 10% of infection belongs to other types of candida which may not cause any symptoms. Another name for vaginal thrush is candidiasis or yeast infection. Over 50% of women will have vaginal thrush at least once in their lifetime and about 5% of women have frequent episodes.
The symptoms of vaginal thrush include:
- Genital itch – this is the most common symptom of thrush. Itching may be especially worse before your period
- Soreness or burning in the vagina during or after sex
- Abnormal discharge – that can be thick and white but sometimes it can appear normal
- A change in the smell of your vaginal secretions
- Redness and inflammation of the genital skin outside the vagina (the vulva)
- Soreness or discomfort on urination
- Pain – particularly if the infection occurs a number of times or hasn’t been treated properly
- Small white spots on the vaginal wall or curds in the discharge
Diagnosis of vaginal thrush is often made based on a number of things including your symptoms, physical examination, examination of vaginal secretions under the microscope and vaginal culture. There are many other conditions of the vagina and vulva that have symptoms in common and even associated with thrush, so if there is doubt about the diagnosis, or when it is recurrent, it is essential that your doctor takes a vaginal swab for laboratory testing before treatment is started.
Treatment with a cream or ovules (pessaries) in the vagina or the use of an oral anti-fungal tablet/capsule are two effective means of treating thrush. There are many different names for these creams and ovules/pessaries (some common examples are miconazole and clotrimazole) and usually they come with an applicator that helps to insert them deep in the vagina. Even if your period starts you can still use these medications. The medication is available from pharmacies and can be used to treat an isolated episode of thrush – that’s one that occurs more than a year since the previous episode (see below for treatment of recurrent thrush).
Vaginal thrush may also be treated with anti-fungal tablets or capsules that you take by mouth, and these medications are best administered under the supervision of your medical practitioner. These are not to be taken by pregnant women.
You should see your doctor if:
- This is the first time you have experienced thrush symptoms
- You are not sure if the problem you have is thrush
- This is the second thrush infection you have had in less than a year
- You are pregnant or breast feeding
- You have not responded to treatment and there is no improvement.
- If symptoms come back in less than a year, or your response to treatment is unsatisfactory, do not self-treat or you risk producing a chronic (ongoing) condition.
When you see your doctor, make sure that the diagnosis is confirmed with a swab sent for laboratory testing. Please note that swabs may not give any useful results if any treatment has been used in the week or two before the test.
The yeast that causes most thrush, candida albicans, can live in the mouth and bowel without causing any problems. It can travel to the vagina from the anus via the perineum – the area between the anus and the vagina. This is known as perineal spread. Other species of yeast often live in the vagina but cause no harm.
Candida albicans causes the most severe symptoms of vaginal thrush.
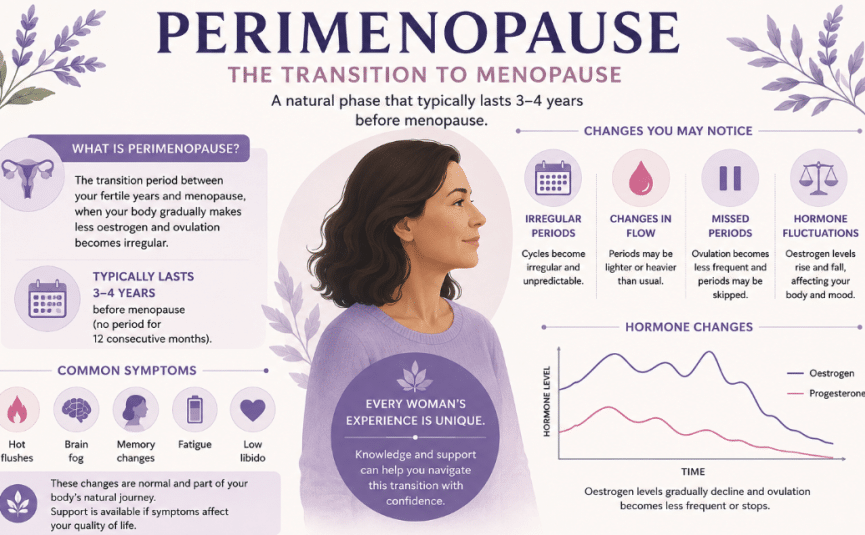
Women are more likely to get vaginal thrush between puberty and the menopause because, under the influence of the hormone oestrogen, the cells lining the vagina produce a sugar. Yeasts (like candida albicans) feed on those sugars. That is why thrush is rare before puberty, in breast-feeding women (who have low oestrogen levels), and after the menopause (unless a woman is on menopausal hormone therapy (MHT) or has diabetes).
Although numerous lifestyle changes have been suggested in the past to prevent thrush (eg: avoiding sugar, tight clothing and alteration of sexual practices), NONE of these have been proven to be effective. Candida albicans is not sexually transmitted.
Antibiotics promote the growth of yeasts by destroying the bacteria that can protect against them, so are best avoided unless really necessary. If you are a diabetic, then good control of blood sugar levels is helpful. Contrary to popular belief, the oral contraceptive pill makes no significant difference to a woman’s chances of getting thrush. The long-acting progestogen contraceptives, Depo-Provera TM (injection) and progesterone releasing rods, however, do lower the incidence of thrush, because they suppress ovarian production of oestrogen and contain no oestrogen themselves. If an oral contraceptive is needed, it is probably best to have one that contains a low oestrogen level. Breast feeding has the same effect, which is why thrush is seldom a problem in breast feeding women.
A small number of women will get thrush a couple of times a year or more. This is called recurrent candidiasis or thrush and is best managed by a doctor with a special interest in this problem.
If you have recurrent vaginal thrush you should never treat yourself. Your doctor should take a vaginal swab with each episode of thrush to monitor your condition. Occasionally tests need to be taken to see whether the candida is resistant to the treatment that you are using. Chronic fungal infections of the vulval skin can occur even with negative swabs.
Treatment choices for recurrent thrush include:
- Combined oral and vaginal azole therapy – this means taking tablets as well as using anti-candida creams inserted in the vagina – medium term (3 weeks)
- Long-term (at least 6 months’) treatment with an oral azole
- A change to a lower oestrogen dose for women taking menopausal hormone therapy (MHT)
- Boric acid made into vaginal pessaries by a compounding chemist.
Thrush is not a sexually transmitted disease. Generally, no benefit is shown by treating the male sexual partner of women with recurrent vaginal thrush. Treatment is recommended for men only when they have symptoms themselves, preferably after swabs have been taken and candida albicans confirmed.
Dr Len Kliman is a member of the International Society for the Study of Vulvovaginal Disease (ISSVD) and the Australian and New Zealand Vulvovaginal Society (ANZUS).
With over three decades of experience, Dr Kliman has treated tens of thousands of gynaecological patients and delivered over 20,000 patients and still counting!
In 2017, Dr Kliman was ordered an Order of Australia for his services to obstetrics and gynaecology.